TLMNI Funded Programmes: Bangladesh
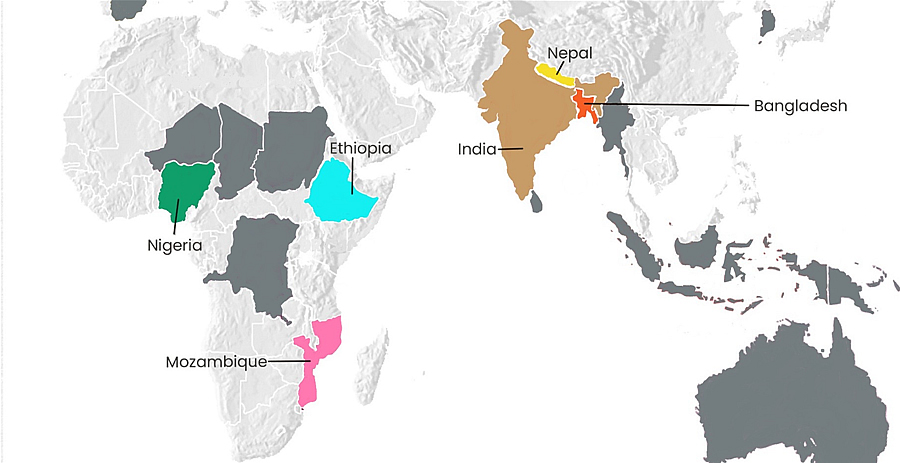
Click on the name of a country on the map or the list below to find out more.
Bangladesh | Ethiopia | India | Mozambique | Nepal | Nigeria
Bangladesh
Leprosy thrives where there is poverty and overcrowding, and these exist side by side in Bangladesh. With more than 1,300 people per square kilometre, Bangladesh has one of the highest population densities in the world. Almost 2 out of every 10 people live in poverty.
Bangladesh has the 4th highest rate of leprosy in the world. In 2024, a further 3,519 people were diagnosed with leprosy in Bangladesh.
Your support is enabling vital work in the following areas to take place in Bangladesh:
Healthcare: Doctors, dermatologists, and other healthcare workers receive training in leprosy detection and case management through TLM activities. Healthcare services are brought directly to communities through awareness sessions and screenings in communities. TLM is also collaborating with the National Leprosy Programme in Bangladesh to expand the roll-out of Single-Dose Rifampicin Post-Exposure Prophylaxis (SDR-PEP) – a tablet that when taken can reduce the risk of someone developing leprosy after being exposed to the disease.
We also support The Leprosy Mission Bangladesh’s DBLM Hospital, the only hospital in the country that provides reconstructive surgery and treatment for leprosy-related complications.
Community Partnerships: Together with The Leprosy Mission Bangladesh, we work with local NGOs, community groups, and government health departments to combat stigma, raise awareness of leprosy, and identify new cases throughout communities in Bangladesh. TLM also aims to strengthen these organisations by building capacity in organisational governance, technical skills and operational effectiveness.
Empowering people and communities: We work to empower people affected by leprosy, so they can support each other and advocate for change. Through self-help groups (SHGs), communities come together to pool savings and provide each other with small loans, with the aim of increasing household incomes and economic resilience.
Research: Our research in Bangladesh includes development of a mobile and rapid diagnostic test for leprosy, methods for early detection of leprosy transmission, and further research into advancing preventative medication for leprosy.
You helped us achieve the following in Bangladesh last year:
- 11,557 people exposed to leprosy received SDR-PEP medication, thus reducing the likelihood of them developing leprosy
- 180 people with disabilities due to leprosy received assistive devices including protective footwear, crutches, and wheelchairs
- Trained Church pastors and leaders applied their training throughout their communities, referring 53 suspected leprosy cases for screening, and visiting 46 households of persons affected by leprosy to provide counselling and follow-up support.
- 217 SHGs with 2,729 members across eight districts (47% of whom are affected by leprosy), built a combined capital base equivalent to £28,904.
- 417 SHG members accessed loans from this capital to initiate or expand income-generating activities, thus increasing economic resilience.